Why is Epidemiology important to Paramedicine?

Figure 24 - Ambulance
Epidemiology in Paramedicine
It is said that Epidemiology sets the foundation that pervades all of health care (Merrill, 2012). By identifying and studying known determinants of specific illnesses, diseases, or events, health care professionals have the ability to prevent that which may affect select populations. This in turn may prevent future illness by recognizing risk factors and in treating patients sooner or before a disease, illness or event occurs or begins it's course. Two sub-disciplines of epidemiology that have a significant impact on the paramedic industry are occupational epidemiological and clinical epidemiology. One focuses on the reduction of workplace hazards and the prevention of occupational injury, the other on the efficacy of screening, diagnosis and treatments in the clinical setting.
Occupational epidemiology is defined as work-related patterns of disease and other adverse health outcomes (Occupational Epidemiology, 2012). With close to a million workplace injuries reported annually in Canada, paramedics themselves fall victim to a wide variety of workplace injuries (Occupational Injuries & Diseases in Canada 1996-2008, 2013). A study of emergency medical service personal conducted in the US found that the overall injury rate to be close to 35% (Maguire, Hunting, 2005). Epidemiology provides critical information regarding occupational injuries trends, allowing for industry managers to find new solutions to address the increasing incidences of injuries. Recent changes include hydraulic ambulances and stretchers, bariatric lifting devices, weight limitations on equipment and exercise programs designed to aid in strengthening lifting muscles. In addition to muscoskeletal injuries, the incidences of burn out, post-traumatic stress, inadvertent needle stick injuries, and the acquisition of communicable diseases can be monitored in order to quickly recognize the need to implement programs such as influenza vaccinations or the creation of a Critical Incident Stress Debriefing team.
Clinical epidemiology attempts to identify the health consequences of a test or treatment (Merrill, 2012). This kind of information can be acquired during daily paramedic operations and can significantly impact the treatment of future patients in the pre-hospital setting. An example is that which is obtained and conducted by the Resuscitation Outcomes Consortium (ROC) trials. Initiated in 2006, The National Institute of Health (NIH), along with other federal and Canadian agencies began research along with 11 hospital and EMS systems located throughout the United States and Canada. Its focus was on pre-hospital cardiopulmonary arrest and severe traumatic injury; two areas in which paramedic interventions are thought to have the most potential for positive outcomes (https://roc.uwctc.org/tiki/tiki-index.php). The large scale trials intended to expand the understanding of new and current treatment philosophies previously supported by smaller studies, thus providing support for widespread use. These Experimental treatments were then compared to previous treatment philosophies with emphasis on cognitive stability - survival greater than 28 days and with return to full mental and physiological capabilities. “…we will know, based on large and well-designed studies, what interventions really make a difference” said COL John Holcomb MD (https://roc.uwctc.org/tiki/tiki-index.php).
ROC trials have included the use of concentrated saline solution in Traumatic Brain Injured patients and patients suffering from shock due to trauma, the use of an impedance threshold device during CPR, early vs. late cardiac defibrillation analysis, real time quality CPR feedback, pause vs. no pause rescue breathing, and amiodarone vs. lidocane use during cardiac arrests. (https://roc.uwctc.org/tiki/tiki-index.php). All of which have had a direct impact in initiating change towards the treatment and management of patients in the pre-hospital setting
Locally, the Toronto group has been named the Toronto Regional Rescunet and includes a network of 9 surrounding areas, who together with ORANGE (the Ontario Area Base Hospital Program with response bases located throughout the province), responds to over 600 000 calls for medical assistance per year (http://www.emergencymedicine.utoronto.ca/research/ptmr/CS/ROC/rescunet.htm).
Observational and clinical epidemiological studies provide valuable information to the paramedic industry by not only ensuring that the treatments they provide are reflective of the most current, credible and up-to-day clinical information, but also by providing information as to the prevalence of occupational injury/disease and a means to attempt its prevention.
It is said that Epidemiology sets the foundation that pervades all of health care (Merrill, 2012). By identifying and studying known determinants of specific illnesses, diseases, or events, health care professionals have the ability to prevent that which may affect select populations. This in turn may prevent future illness by recognizing risk factors and in treating patients sooner or before a disease, illness or event occurs or begins it's course. Two sub-disciplines of epidemiology that have a significant impact on the paramedic industry are occupational epidemiological and clinical epidemiology. One focuses on the reduction of workplace hazards and the prevention of occupational injury, the other on the efficacy of screening, diagnosis and treatments in the clinical setting.
Occupational epidemiology is defined as work-related patterns of disease and other adverse health outcomes (Occupational Epidemiology, 2012). With close to a million workplace injuries reported annually in Canada, paramedics themselves fall victim to a wide variety of workplace injuries (Occupational Injuries & Diseases in Canada 1996-2008, 2013). A study of emergency medical service personal conducted in the US found that the overall injury rate to be close to 35% (Maguire, Hunting, 2005). Epidemiology provides critical information regarding occupational injuries trends, allowing for industry managers to find new solutions to address the increasing incidences of injuries. Recent changes include hydraulic ambulances and stretchers, bariatric lifting devices, weight limitations on equipment and exercise programs designed to aid in strengthening lifting muscles. In addition to muscoskeletal injuries, the incidences of burn out, post-traumatic stress, inadvertent needle stick injuries, and the acquisition of communicable diseases can be monitored in order to quickly recognize the need to implement programs such as influenza vaccinations or the creation of a Critical Incident Stress Debriefing team.
Clinical epidemiology attempts to identify the health consequences of a test or treatment (Merrill, 2012). This kind of information can be acquired during daily paramedic operations and can significantly impact the treatment of future patients in the pre-hospital setting. An example is that which is obtained and conducted by the Resuscitation Outcomes Consortium (ROC) trials. Initiated in 2006, The National Institute of Health (NIH), along with other federal and Canadian agencies began research along with 11 hospital and EMS systems located throughout the United States and Canada. Its focus was on pre-hospital cardiopulmonary arrest and severe traumatic injury; two areas in which paramedic interventions are thought to have the most potential for positive outcomes (https://roc.uwctc.org/tiki/tiki-index.php). The large scale trials intended to expand the understanding of new and current treatment philosophies previously supported by smaller studies, thus providing support for widespread use. These Experimental treatments were then compared to previous treatment philosophies with emphasis on cognitive stability - survival greater than 28 days and with return to full mental and physiological capabilities. “…we will know, based on large and well-designed studies, what interventions really make a difference” said COL John Holcomb MD (https://roc.uwctc.org/tiki/tiki-index.php).
ROC trials have included the use of concentrated saline solution in Traumatic Brain Injured patients and patients suffering from shock due to trauma, the use of an impedance threshold device during CPR, early vs. late cardiac defibrillation analysis, real time quality CPR feedback, pause vs. no pause rescue breathing, and amiodarone vs. lidocane use during cardiac arrests. (https://roc.uwctc.org/tiki/tiki-index.php). All of which have had a direct impact in initiating change towards the treatment and management of patients in the pre-hospital setting
Locally, the Toronto group has been named the Toronto Regional Rescunet and includes a network of 9 surrounding areas, who together with ORANGE (the Ontario Area Base Hospital Program with response bases located throughout the province), responds to over 600 000 calls for medical assistance per year (http://www.emergencymedicine.utoronto.ca/research/ptmr/CS/ROC/rescunet.htm).
Observational and clinical epidemiological studies provide valuable information to the paramedic industry by not only ensuring that the treatments they provide are reflective of the most current, credible and up-to-day clinical information, but also by providing information as to the prevalence of occupational injury/disease and a means to attempt its prevention.

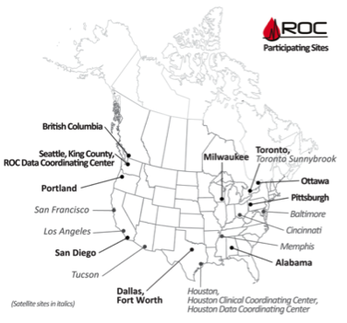

Figure 27 - ROC Rescue Net Participating Regions
